
INTRODUCTION
Worldwide, both physical and mental health has been affected by the current COVID-19 pandemic[1]. Cardiac implantable electronic devices (CIEDs), such as pacemakers, implantable cardioverter-defibrillators (ICD), cardiac resynchronization therapies, are standard of care in life-threatening arrhythmias, and device implantation rates show a yearly increase[2][3]. Individuals living with CIEDs not only have multiple underlying diseases, but also experience quality of life changes[4][5][6]. These patients are vulnerable to get severe COVID-19 symptoms and to develop emotional distress. Therefore, an online purpose designed questionnaire was developed to assess their physical and mental health condition during the pandemic. In the current paper, a multivariate analysis based on a principal axis factoring (PAF) was performed focusing on CIEDs patients’ concerns related to: device functioning, having received a shock (if ICD), the possibility to receive a shock (if ICD), access to medical care, reaching physicians, access to medication, getting infected by SARS-CoV-2, health of caretakers, health of patients’ loved ones. PAF is part of the Exploratory Factor Analysis (EFA) class, which is frequently used in healthcare research[7][8][9][10]. One of the most difficult problems in EFA lies in the identification of the optimal number of factors[11][12][13][14], as an inappropriate number of factors may lead to imprecise conclusions. A previous paper[15] highlighted the importance of the total cumulative variance explained by the factors in the establishment of the appropriate number of factors. It was proved that, at least, a threshold value of cumulative variance should be explained by the extracted factors, considering the specificity of the research. Based on the mentioned previous research, and on a thorough scientific literature review, we propose three rules to be considered in selecting the best-fitted number of factors, as well as an additional rule, for verification purposes, of the selected number of factors
MATERIAL AND METHOD
A purpose-designed questionnaire containing 45 multiple choice questions was created to assess CIED patients’ mental concerns and physical health condition during the COVID-19 pandemic. The questionnaire was completed online, anonymously and voluntarily by 210 CIEDs patients from the outpatient care of the Institute for Cardiovascular Emergencies and Transplant and by international patients, as part of online support groups mainly from the USA, UK, Hungary, Canada. Eighteen participants were excluded due to contradictory responses. The final data analysis included 184 responses. The varimax method for rotation in EFA was proposed by Kaiser, which is one of the most frequently used methods of rotation[16]. PAF was performed, applying the varimax orthogonal rotation method focusing on the concerns of the respondents. Initially, the study included 9 variables (Var): Var1- device functioning, Var2- having received a shock (if ICD), Var3- the possibility to receive a shock (if ICD), Var4- access to medical care, Var5- reaching physicians, Var6- access to medication, Var7- getting infected by SARS-CoV-2, Var8- health of caretakers, Var9- health of their loved ones. A preliminary study excluded Var3, Var9 due to their low variability. Further communality analysis excluded Var1, Var2, and Var8. The exclusion of Var2 and Var3 is explained theoretically by the fact that these concerns may arise only for patients with ICD, not for every CIED patient assessed in the current study. PAF was performed on the remaining variables: Var4, Var5, Var6, Var7. Based on an in-depth study of the scientific literature, and considering the results of the research mentioned anteriorly[15], we suggest the following three rules to determine the number of extracted factors: • rule 1): the total explained variance to be at least 60 %-65 % – established since none of the variables passed the normality assumption, • rule 2): the extracted eigenvalues to be at least 1, criteria proposed by Kaiser[16], • rule 3): visual interpretation of the Scree plot, called as Cattell’s Scree test[17]. Parallel analysis (PA) was proposed by Horn, named as the Monte Carlo simulation method, useful to determine the number of factors, which should be extracted in EFA[18]. One of the reasons that it is less utilized in research is due to the fact that it requires heavy computational resources. However, we propose a Monte Carlo Parallel Analysis as an additional verification step, after establishing the appropriate number of factors.
RESULTS AND DISCUSSION
The eligible 184 responses were registered from geographically different points of the world, mainly from Europe (Romania, Hungary, UK, Ireland, Switzerland, Slovakia, Spain) and the USA; all respondents were patients living with cardiac implantable electronic devices. Table 1 presents the correlation coefficient (r) matrix, and the corresponding significance (sig) of each correlation. Values below 0,05 (sig<0,05) indicate significant correlation.
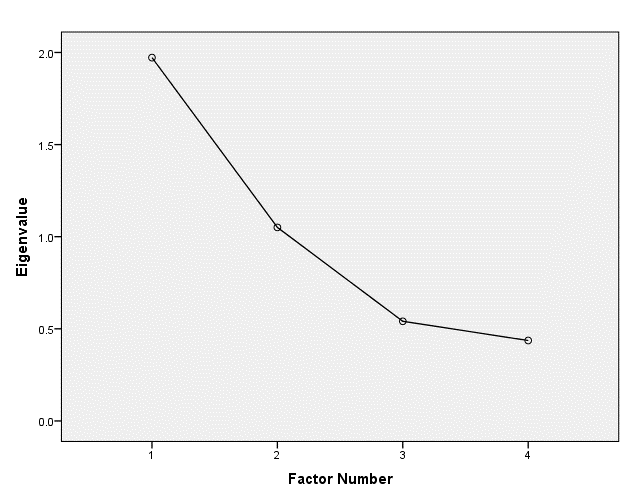
Table 2 presents the obtained eigenvalues, variance explained by each prospective factor, and the total cumulative variance explained. Corresponding to Rule 3, the Scree plot was created, which is a line plot showing the eigenvalues of factors used to determine the number of factors to retain in PAF (Fig.1). Based on this visual interpretation and on Rule 2 (the eigenvalue of each selected factor must be at least 1) two factors were chosen. Furthermore, during this process the total cumulative variance explained by the two selected factors (marked with * in the table) was 75,56 %, as presented in Table 2.
| Factor | Initial Eigenvalues | ||
| Eigenvalue | % of Variance | Cumulative % | |
| *Factor1 | 1,97 | 49,3 | 49,3 |
| *Factor2 | 1,05 | 26,26 | 75,56 |
| Factor3 | 0,54 | 13,52 | 89,08 |
| Factor4 | 0,43 | 10,92 | 100 |
Table 3 presents the result of the Bartlett’s Test of Sphericity (BTS). BTS indicates significant findings. We suggest BTS application at the 0,05 significance level. The obtained small value of the significance, 0 (0<0,05), indicates that the factor analysis can be applied on the considered data. Furthermore, the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) was applied. KMO should indicate non-significance. We suggest KMO application at the 0,05 significance level. The obtained result was 0,636 (0,636>0,05), which indicates an appropriate application of the exploratory factor analysis.
Table 4 presents the communalities: initially and after extraction. All variables are appropriate as their communality values after the extraction is greater than the threshold (0,263).
| Variables | Initial | Extraction |
| Var4 (access to medical care) | 0,295 | 0,393 |
| Var5 (reaching physicians) | 0,353 | 0,641 |
| Var6 (access to medication) | 0,361 | 0,61 |
| Var7 (getting infected by SARS-CoV-2) | 0,064 | 0,263 |
Table 5 shows the results of the two identified factors. Variables loaded with the absolute value lower than 0,3 were removed. Low values were considered as redundant.
| Factor | ||
| 1 | 2 | |
| “Healthcare-related concerns” | “Fear of COVID-19” | |
| Var4 | 0,77 | |
| (access to medical care) | ||
| Var5 (reaching physicians) | 0,73 | |
| Var6 (access to medication) | 0,62 | |
| Var7 (getting infected by SARS-CoV-2) | 0,51 | |
According to the additional verification step, we performed the Monte Carlo Parallel Analysis (PA) with the following parameters: number of variables: 4; number of subjects: 184; and number of replications: 1000. Table 6 presents the obtained results: in the first column the Eigenvalue, in the second the Random Eigenvalue (RE) and in the last one the Standard Deviation (SD). The obtained simulation result indicates the extraction of two factors as follows: the eigenvalue of the first factor should be at least 1,153, and the next factor should have at least the eigenvalue of 1,042. According to Table 2 the eigenvalue of the first factor is 1,972, which is a higher value than 1,153 obtained by PA. The eigenvalue of the second extracted factor is 1,051 that is higher than the value 1,042 obtained by PA. Therefore, the results of PA confirm the correctness of extracting the two factors.
| Eigenvalue | RE | SD |
| 1 | 1,153 | 0,045 |
| 2 | 1,042 | 0,032 |
| 3 | 0,96 | 0,036 |
| 4 | 0,844 | 0,054 |
Factor 1 was loaded with Var5, Var6, and Var7, indicated in column 1, with the values of 0,772, 0,773, 0,624. All these variables, access to medical care, medication, and contact physicians, are vital components of an appropriately working healthcare system. Thus, Factor 1 was defined as “Healthcare-related concerns”, to emphasize that CIEDs patients worry about their basic medical care, which is currently affected by the COVID-19 pandemic. Individuals living with CIEDs are part of a vulnerable group of chronic patients. Providing them accurate information about healthcare is crucial, as they have to attend follow-up visits on a regular basis, in order to check device functioning and prevent health deterioration[6]. Multiple studies show that emotional support and patient education improves quality of life; with the recent rapid digital transformation in healthcare, cardiologists, electrophysiologists, and physicians in training can provide online and/or telephonic support to high-risk patients adding practical and psychological benefits[19][20][21]. Factor 2 was loaded with Var7, with the value of 0,512, indicated in column 2 of Table 5. This factor was defined as “Fear of COVID-19”. The fact that Factor 2 has only one component underlies Var7’s independent and major effect on the respondents’ life, which is consistent with medical literature. COVID-19 independently influences mental health, which might be due to the fear of getting infected by SARS-CoV-2, and to the daily media coverage and misinformation on social media. Platforms providing misinformation should be removed and official sources should provide and disseminate information about preventive measures for everyday life with cardiac devices and healthcare assistance during times of a pandemic[1][22][23].
CONCLUSION
Our study described a multivariate analysis called PAF, part of the EFA class, which is frequently used in healthcare research. PAF was performed on CIEDs patients’ concerns during the COVID-19 pandemic. In order to extract the optimal number of factors, which is one of the most difficult problems in EFA, we considered three principal rules, and an additional step to verify the correctness of the number of factors. The two extracted factors were explained by 75,56 % of the cumulative variance. Factor 1 was defined as “Healthcare-related concerns” and Factor 2 as “Fear of COVID-19 disease”, which highlights the current concerns of CIEDs patients. Consequently, the need for accurate medical information provision, patient education and support are emphasized in order to improve healthcare during the pandemic. The Social Network of Machines (SOON) project aims to investigate a solution based on the use of autonomous social agents to optimize the complex manufacturing processes in the framework of Industry 4.0. In the current article we performed an experimental study on the collected data of CIEDs patients. The approach was based on statistical modeling. As a future research, the statistical modeling presented in the current paper together with other methods of data science and artificial intelligence will be applied for industrial data analysis available in the framework of the SOON project.
ACKNOWLEDGMENTS
This study was developed in the framework of the CHIST-ERA program supported by the Future and Emerging Technologies (FET) program of the European Union through the ERA-NET Cofund funding scheme under the grant agreements, title: Social Network of Machines (SOON). This research was supported by a grant of the Romanian National Authority for Scientific Research and Innovation CCDI-UEFISCDI, project number 101/2019, COFUND-CHISTERA-SOON, within PNCDI III. We would like to thank the “Advanced Research in Information Technology” Research Center (CARIT) and the Electrophysiology Team of the Emergency Institute for Cardiovascular Disease and Transplant (IUBCvT) Targu Mures for their support.