
Introduction
The total testing process starts with the clinical question, followed by test selection, order, sample collection, sample transportation, test measurement, result reporting, clinical answer and clinical action. It finishes with the effect of patient care (1). The physician’s attention is logical when the test result is out of reference ranges or exceeds decision values. Considering a pathological state when the test results are falsely normal is more difficult. The intracellular potassium concentration is about 140-150 mmol/L, while plasma physiological concentration is 3.5-5.0 mmol/L (2). Potassium can be released from blood cells during sample collection, transportation, clotting and centrifugation. The most common cause of potassium leakage from blood cells is hemolysis. It may result from inappropriate collection needles, intravenous catheter blood collection, syringe draw, traumatic draw, extended tourniquet time, vigorous mixing of tubes, agitation during transport and underfilling (3). Automated analyzers measure the hemolysis index in all serum/plasma laboratory samples. Visual assessment of hemolysis is not recommended and can seriously jeopardize patient safety (4). Falsely elevated blood potassium may also be caused by pumping with the fist, low-temperature whole blood storage, long storage times, hereditary pseudohyperkalemia, thrombocytosis, leukocytosis, etc. (3). It is a challenge for laboratories to detect falsely elevated potassium results if it is not caused by hemolysis.
Missed and left untreated pseudonormokalemia could lead to dangerous situations resulting from hypokalemia, such as cardiac arrhythmias (5).
This case study aims to present a patient with pseudonormokalemia, true hypokalemia. A 50-year-old male was admitted to the Department of Internal Medicine due to sepsis from a dental infection. He had Addison‘s disease, hypothyroidism, asthma, depression and penicillin allergy. His regular medication included Hydrocortisone 10 mg 2-1-0, Levothyroxine 50 µg 1.5-0-0, Mirtazapine 45 mg 0-0-0-1, and budesonide-formoterol inhalation. Upon admission, a physical examination revealed a blood pressure of 115/70, a regular heart rate of 110/min, vesicular breathing, a body temperature of 38.9 °C and a body mass index of 29.6 kg/m2. The basic biochemistry tests, including electrolytes, were collected.
The patient signed informed consent for the publication of his case study. The publication was approved by the local Tomas Bata Hospital Ethics Committee.
Laboratory analyses
The basic biochemistry tests during antibiotic treatment showed normokalemia. The blood collection was performed in the morning at 6.00 and serum indices showed no hemolysis (free hemoglobin was 0.00 g/L), lipemia or icterus. The blood count revealed thrombocytosis and anemia. All tests are displayed inTable 1.
The serum sample was drawn in a 6 mL VACUETTE red top tube with clot aktivator (Greiner Bio-One Gmbh, catalog number 476092, Kremsmunster, Austria). The 10-minute centrifugation at 1500xg was done within one hour after sampling. Our laboratory performs two checks when reporting laboratory test results. Biomedical scientists perform the technical validation, which includes evaluating the impact of serum indices and other preanalytical factors on laboratory test results. The medical validation is performed by specialists in laboratory medicine and it covers the consideration of the clinical plausibility of all results. If a patient has thrombocytosis over 500x109/L, pseudohyperkalemia or pseudonormokalemia is considered (6). The plasma potassium measurement in whole blood or a lithium heparin tube is recommended by the written interpretative comment on the result report.
Further investigation
The lithium heparin plasma sample was collected at 9.40, the results were available in 51 minutes and revealed hypokalemia. All plasma results are shown inTable 2.
| Laboratory test | Result | Reference interval |
|---|---|---|
| Na (mmol/L) | 137 | 136-144 |
| K (mmol/L) | 2.9 | 3.5-4.8 |
| Cl (mmol/L) | 106 | 95-107 |
| Mg (mmol/L) | 0.83 | 0.80-0.94 |
| Na - sodium. K - potassium. Cl - chloride. Mg - magnesium. | ||
The plasma sample was measured in a 3 mL green top lithium heparin tube from the same manufacturer (catalog number 454082). The same centrifugation conditions were used as for serum sample. All biochemical tests were measured on Abbott Architect analyzer ci 16200 (Abbott Laboratories, Illinois, USA). This situation can be concluded as pseudonormokalemia. The thrombocytosis was temporary. After the successful antibiotic treatment of sepsis, the thrombocyte count was 242x109/L and serum potassium concentration was 4.2 mmol/L. Results before hospital discharge are shown inTable 3. The thrombocyte count decreased due to the successful treatment of inflammation and potassium concentration increased after substitution therapy.
What happened?
The patient initially had thrombocytosis and normal serum potassium concentrations. Results are shown inTable 1. Plasma potassium measurement revealed hypokalemia of 2.9 mmol/L. All results are visible inTable 2.
We have seen the difference between serum and plasma potassium concentrations of 1.1 mmol/L.
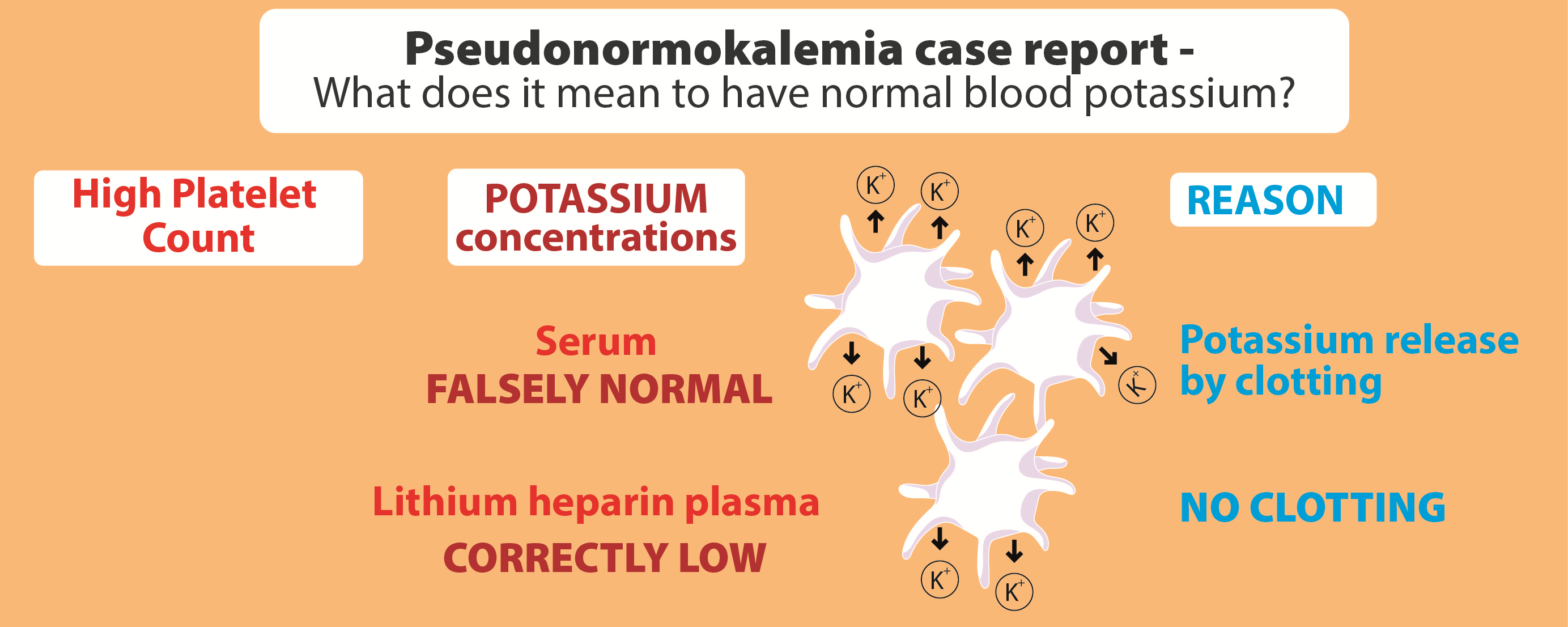
In this case, the elevated serum potassium may result from its release from platelets and other cells during clotting. The impact of high platelet numbers on potassium results is only seen in serum, and falsely elevated potassium results can be identified by comparing the results to heparin plasma values.
Discussion
This case study describes a case study of pseudonormokalemia, true hypokalemia, probably due to thrombocytosis. The physiological difference in potassium concentration between plasma and serum is no more than 0.3 mmol/L (7). The cut-off for pseudohyperkalemia, the difference between serum and plasma concentrations, was defined as 1.0 mmol/L (8). Whole blood was suggested for plasma potassium measurement on blood gas analyzers (8). On these instruments, the undetectable hemolysis is a real potassium measurement problem, which is why plasma is the better choice. The hemolysis detection on these devices may be available in the future. Lithium-heparin plasma after centrifugation is another option; it is the easiest way to identify falsely elevated potassium results caused by thrombocytosis (9). The diagnosis of pseudonormokalemia is an even more significant challenge compared to pseudohyperkalemia. Delgado et al. reported that up to 0.14% of the total serum potassium determinations were susceptible to pseudohyperkalemia or pseudonormokalemia. Pseudonormokalemia accounted for 85% of cases (10). We can conclude that pseudonormokalemia was also presented in this case study.
What YOU should / can do in your laboratory to prevent such errors
The best way to eliminate this phenomenon is to change towards heparin-plasma as the standard material completely. Interpretative comments in patients with thrombocytosis over 500x109/L recommending plasma potassium measurement are helpful even in patients with normal serum potassium values. This comment may be added to all reports with thrombocyte results over 500x109/L. It explains that the patient has probably falsely elevated serum potassium results and recommends the lithium heparin plasma sample collection for potassium measurement.