
1. Introduction
Healthy diet represents not only the adequate intake of energy and nutrients from the desired food groups, but also the intake of fluids and their sources through various beverages and foods. According to the scientific opinion of the European Food Safety Authority (EFSA), depending on age, water accounts for between 55% and 75% of body mass and is involved in many physiological processes (EFSA, 2010). Therefore, to maintain fluid homeostasis and support physiological functions, it is necessary to consume an adequate amount of fluid. Good management of fluid intake in children is particularly important because it can affect cognitive function and, consequently, academic performance (Bar-David et al., 2005; Perry et al., 2015; Fuchs et al., 2016; Bottin et al., 2019; Suh and Kavouras, 2019).
According to the recommendations of the EFSA, children aged 4 to 8 should consume 1600 mL of fluid per day, 20% of which should come from food and 80% from beverages, with the main choice of beverage being water (EFSA, 2010). Despite existing recommendations, it is observed that most children in Europe do not consume enough fluids (Guelinckx et al., 2015; Suh and Kavouras, 2019; Mesana Graffe et al., 2020).
The contribution of the various fluid sources to the total daily fluid intake also varies widely. Here, water contributes between 17% and 84% of total daily fluid intake (Guelinckx et al., 2015; Suh and Kavouras, 2019). Furthermore, the fact that children are increasingly consuming beverages with added sugar is certainly of concern, and it is well known that excessive consumption of these beverages increases the risk of developing obesity, metabolic syndrome, and tooth decay (Guelinckx et al., 2015; Bottini et al., 2019; Farhangi et al., 2022; Ooi et al., 2022).
To the author's knowledge, there are no relevant data on fluid intake and beverage composition in primary school-aged children in Croatia. In addition, it is extremely interesting to observe the contribution of beverages to daily energy intake and added sugar intake, considering that in a national sample of 5,591 children aged 7 to 9, more than 1/3 were estimated to have increased body weight or to be obese (Musić Milanović et al., 2020).
It is certainly necessary to point out that there are no recommendations for fluid intake in the Croatian national guidelines for the nutrition of school-age children (Capak et al., 2013). However, it is mentioned that the appropriate source of fluids is water and that drinking water should be available for all children. It is also recommended that tea and cocoa drinks should be consumed with as little sweetener as possible and that they should be sweetened with honey instead of sugar if necessary.
Accordingly, the aim of this study was to determine the total fluid intake and beverage consumption of school-aged children in Croatia. In addition, the aim was to estimate the contribution of beverages to the daily energy and added sugars intake.
2. Materials and methods
Study design and population
This study was designed and conducted as a cross-sectional observational study (school year 2019/2020) in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the School of Medicine, University of Zagreb (380-59-10106-19-11/307). Approvals for the implementation of the pilot project in primary schools were obtained from the relevant institutions (Ethics Committee of the Institute for Medical Research and Occupational Health: 100-21/16-8; the Croatian Ministry of Science and Education and the Education and Teacher Training Agency: 602-01/16-01/00388).
The study takes place within "Pilot project: school meals and fruit and vegetable intake in schools with and without a garden", which is part of the Horizon 2020 project "Strengthening European Food Chain Sustainability by Quality and Procurement" (Strength2Food, H2020-SFS-2015-2, contract no. 678024). Consequently, the selection of schools and recruitment of children were done according to the protocol of the project (Colić Barić et al., 2021). Of the selected 14 elementary schools in the city of Zagreb, 681 children had consented in writing to participate in the study.
The data analysis was carried out using the per-protocol approach on a total of 195 second grade children with a median age of 8.8 years (28.6% of the study sample; 52% boys) who completed 3-day dietary protocols. It was estimated that at least 142 children from the population of second graders in 14 selected primary schools were needed to achieve an 80% confidence level that the actual value was within ± 5% of the measured value (Suresh and Chandrashekara, 2012).
Dietary assessment
Dietary records from 3 non-consecutive days (2 weekdays and 1 weekend day) were used to estimate children's fluid intake from foods and beverages. Following detailed instructions, parents kept records of their children's diets and reported the amount of food and beverages consumed in grams by weighing or measuring them using standard kitchen utensils. To estimate energy and added sugar intake from food and beverages, dietary records were analyzed using the Prehrana software (Infosistem d.d, Zagreb, Croatia), which is based on Croatian food composition tables (Kaić-Rak and Antonić, 1990) and supplemented with food nutrition labelling. In addition, the Danish composition tables were used to evaluate the content of added sugars in children’s diets (National Food Institute, Technical University of Denmark, 2019).
Total fluid intake included fluid from foods and beverages and was compared with the EU Dietary Reference Values (EFSA, 2010). Furthermore, beverages were classified into seven categories: (1) water (fresh, tap, and mineral); (2) milk; (3) milk with added sugar (cocoa, chocolate milk, shake); (4) tea without added sugar; (5) tea with added sugar; (6) 100% fruit and/or vegetable juices; (7) soft drinks (non-carbonated or carbonated water-based flavored drink, 100% fruit and/or vegetable juices with added sugar, instant drinks, drinks made with fruit syrup).
Anthropometric measurements
Anthropometric assessment was performed during Physical Education and Health classes with children wearing light athletic clothing according to standard protocols. Height and weight were measured with a combined medical digital scale and stadiometer (Seca, type 877-217, Vogel & Halke Gmbh & Co., Hamburg, Germany) to the nearest 0.1 cm, and weight to the nearest 0.1 kg, respectively. Body mass index (kg/m2) was calculated from height and body weight data.
The age- and sex-standardized World Health Organization (WHO) z-scores were determined for each child using the AnthroPlus software (Blössner et al., 2009).
Statistical analysis
All analyses were performed using IBM SPSS Statistics v. 23.0, released in 2015 (IBM SPSS Statistics for Windows, Armonk, NY, USA: IBM Corp.). All categorical variables were reported as percentages, while continues variables were presented as median and interquartile range, due to their skewness according to the Shapiro-Wilk normality test. The significance level was set at p < 0.05.
3. Results
Total daily fluid intake was observed in n = 195 children, of whom 52% were boys and 48% girls, with a mean age of 8.8 (8.6 - 9.1) years. The descriptive statistics of the anthropometric measurements presented in Table 1 showed that the children had an adequate weight status.
Regarding dietary intake (Table 1), the children had an average daily energy intake of 1762 kcal (1455 kcal - 1983 kcal), of which carbohydrates accounted for 49.1% of the total daily energy intake, fat for 36.4%, and protein for 15.6%. In addition, the children in the present study had an adequate intake of added sugars (Table 1).
Table 1. Anthropometric characteristics and nutrient intake of children in the total sample1
1All continuous variables are presented as median (interquartile range) and categorical variables as percentages.
The average daily fluid intake of children was 1168 mL (859 - 1563), which is approximately 70.0% (53.7% - 97.7%) of the EFSA recommendation. Furthermore, only 14.4% of children achieved the EFSA reference value for total daily fluid intake. Apart from the total daily fluid intake, this study shows the contribution of foods and different types of beverages to daily fluid intake (Figure 1). Namely, the average of 59.6% of total fluid intake comes from beverages and 40.4% from food. Furthermore, as it is presented in Figure 1, children consumed water the most (34.7% of fluid intake from beverages), followed by soft drinks (6.3% of fluid intake from beverages) and milk (6.1% of fluid intake from beverages).
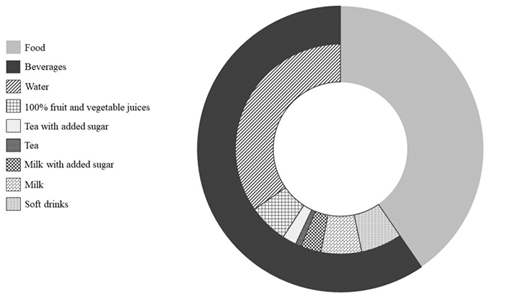
Figure 1. Relative contribution of different source of fluid to the total daily fluid intake. The external circle account for the percentages of fluid from food and beverages, while internal for the contribution of the beverages of each beverage category.
In the present study, children had, on average, 118 kcal (62 kcal – 179 kcal) from the beverages. Taking into account the energy value of the beverage (Figure 2), milk (2.7% of daily energy intake) contributes the most to daily energy intake from beverages, followed by soft drinks (2.5% of daily energy intake) and milk with added sugar (1.9% of daily energy intake) (Figure 2). In the present study, the consumption of 100% fruit and/or vegetable juices in children contributes 0.6% to daily energy intake.
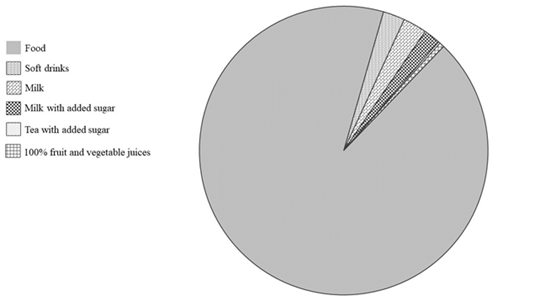
Figure 2. Distribution of daily energy intake from beverages and food
Children consume, on average, about 33.7 g (21.9 g - 49.1 g) of added sugar, of which, on average, 73.5% comes from food and 26.5% from beverages (Figure 3). Of the beverage groups observed, three are profiled as sources of added sugar and these are milk with added sugar, tea with added sugar, and soft drinks. The soft drink group contributes the most to the daily intake of added sugars (19.7%).
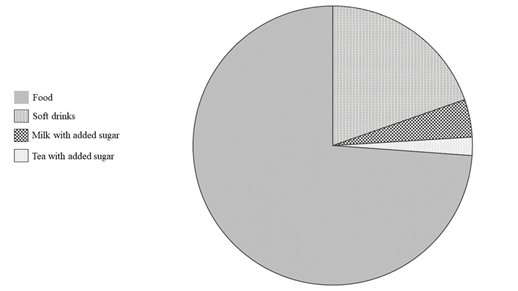
Figure 3. Distribution of daily added sugar intake from beverages and food.
4. Discussion
In line with the objective, the results of the study present the fluid intake of children of primary school age. The findings raise awareness of inadequate fluid intake management in children and point out the need to change their drinking habits.
According to EU dietary reference values, children should consume 1600 mL of fluid per day (EFSA, 2010). Total fluid intake included fluid from foods and beverages. The majority of children (85.4%) in the present study did not reach the reference values for fluid intake, as in other European studies (Maffeis et al, 2016; Vieux et al., 2016; Michels et al, 2017; Vieux et al., 2017). For example, the lowest total fluid intake was observed in 8- to 13-year-old children in Belgium. There, children consumed a total of about 911 mL of fluid and 88% of them did not meet the EFSA recommendations (Michels et al, 2017). Although still insufficient, daily fluid intake is estimated to be somewhat higher in children from France, England, and Italy (Maffeis et al, 2016; Vieux et al., 2016; Vieux et al, 2017). In France, children aged 4 to 13 daily consumed 1324 mL of total water, composed of plain water, water from beverages, and water from solid foods. Furthermore, only 7% to 11% of children complied with EFSA recommendations (Vieux et al., 2016). A similar situation was observed in United Kingdom in children aged 4-13, where total water intake was 1338 mL and only 11.3% of children met EFSA recommendations (Vieux et al., 2017). In addition, normal-weight children in Italy had an average of 1200 mL of total fluid intake per day (Maffeis et al., 2016). In contrast, children in Greece (8 to 14 years), Poland (4 to 10 years), Portugal
(7 to 11 years), Spain (4 to 10 years), and Turkey (4 to 10 years) had higher daily fluid intakes than recommended by EFSA (Guelinckx et al., 2015; Padrão et al., 2016; Bougatsas et al., 2018;).
The result from the present study revealed that children had disproportionate fluid intake from foods and beverages according to the EFSA recommendations (EFSA, 2010). Namely, it has been recommended that beverages of all types contribute up to 80% of the intake of total daily fluid intake (EFSA, 2010), while children in the present study had only 59.6%. A similar disproportion was estimated in children from France and England, where plain water and drinks accounted for 60% and 67%, respectively, of children’s total water intake (Vieux et al., 2016; Vieux et al., 2017). When looking at the different sources of fluids, the three most common beverage groups were water, soft drinks and milk. The proportion of different types of beverages in children's total daily fluid intake differed in studies from EU countries (Vieux et al., 2016; Vieux et al., 2017). In France, water contributes 33% of total daily water intake, while the least coffee and tea, juice-based beverages, sports drinks and flavoured water (< 1%). Soda, 100% fruit juices and fruit drinks contribute 5.3%, 5.5% and 1.2%, respectively, to total daily water intake (Vieux et al., 2016). In England, children had similar intake of water (256.7 mL) and fruit drinks (242.1 ml), followed by milk (212.3 mL), juices (91.8 mL), and soda (89.3 mL) (Vieux et al., 2017). A greater distribution of water (> 60% of total fluid intake) among beverages was found in children from Greece, Belgium and Italy (Maffeis et al., 2016; Michels et al., 2015; Bougatsas et al., 2018). According to the recommendations, it is necessary that the main daily source of fluid is water and that increased consumption of sugar-sweetened beverages may increase the prevalence of obesity and other non-communicable diseases in children (EFSA, 2010; Derén et al., 2019; Malik and Hu, 2022). Since there is no explicit recommendation for the consumption of sugar-sweetened beverages, it is recommended that their consumption should be minimized through appropriate environmental changes, national policies, and education of children and parents. In addition, since they contribute to sugar intake, they should not exceed 10% of daily energy intake from the sugar, together with other foods and beverages (WHO, 2015; Derén et al., 2019).
The second aim of the present study was to determine the contribution of beverage consumption to the daily energy and added sugar intake. The children had an average daily energy intake of 1762 kcal
(1455 kcal - 1983 kcal). This is slightly lower than the national dietary guidelines for primary school children, which recommend an intake of 1855 kcal (Capak et al., 2013). The children had on average 7.7% of daily energy intake from the beverages. This result is consistent with the findings of previous studies in children from France (aged 4 to 13 years) and Italy (aged 7 to 11 years), where beverage consumption accounts for 10.8% of daily energy intake (189 kcal) and 7.1% of daily energy intake
(129.5 kcal), respectively (Maffeis et al., 2016; Vieux et al., 2016). As water and tea do not contribute to daily energy intake, because they have no energy value, it is not surprising that in the current study milk contributes the most to daily energy intake from beverages, followed by soft drinks, milk with added sugar, 100% fruit and vegetable juices and tea with added sugar. Although milk and soft drinks provide energy, milk provides some important nutrients such as vitamin D, riboflavin, potassium and calcium that can maintain health, while soft drinks have no nutritional value. Milk with added sugar, also called flavoured milk, has similar nutritional value to milk but is less desirable in children’s diets because of the sugar content (Gutierrez et al., 2022). In addition, 100% fruit and/or vegetable juices are included in the fruit and vegetable food group as defined by WHO (Agudo, 2005), it is recommended that their consumption be limited (WHO, 2006; Heyman et al., 2017). According to WHO, children aged 7 to 18 years can consume up to 100 mL of fruit juice as one serving of fruit within the five-serving recommendation per day (WHO, 2006), while the American Academy of Pediatrics recommends consumption of 100–130 mL of fruit juices per day for children (Heyman et al., 2017). The results of the present study show that the consumption of 100% fruit and vegetable juices is within the recommended range and that their consumption does not pose a risk for maintaining health. The consumption of tea with added sugar and sweeteners was low and was only observed in children who consumed it for school breakfast. Therefore, it had no major influence on daily energy intake.
Finely, the children consumed an average of 32.2 g (32.2 g – 46.7 g) of added sugar per day, which corresponds to the recommendations of the WHO. However, it would be better if it was reduced below 5%, as WHO conditionally recommends (WHO, 2015). Beverages account for a quarter of daily sugar consumption, with soft drinks being the predominant beverage group. In a recent international meta-analysis, current consumption of beverages with added sugars was estimated to be 38% to 75% of sugar intake in children and 62% to 124% in adolescents, which is more than in the present study (Ooi et al., 2022). In addition, the children in the present study consumed three times less added sugar than the sample of the European multicenter cohort study of children aged 2 to 9 years, who consumed more added sugar from soft drinks and milk than from candy and sweets (Mesana Graffe et al., 2020). The question if sugar-sweetened beverages contribute to the development of childhood obesity is highly controversial. There is evidence that excessive consumption of sugar-sweetened beverages increases the risk of obesity in children. However, children who consume large amounts of sugar-sweetened beverages often have poorer eating habits and lifestyles, which may further influence the development of childhood obesity (Farhangi et al., 2021).
One of the limitations of the study was the accurate ability to assess fluid intake, as children at this age are beginning to consume food and beverages outside of parental care and parents do not have full insight into what children are eating and drinking throughout the day (Livingstone and Robson, 2000; Livingstone et al., 2004). However, the weighed and estimated dietary records used in the present study are considered appropriate for the assessment of total fluid intake in young children aged 5 to 8 (Warren et al, 2018). In addition, the limitation of the study is the incompleteness of the chemical composition tables, which may be limiting for some nutrients such as added sugars, which could lead to an underestimation of these in the beverages (Greenfield and Southgate, 2003).
5. Conclusion
The results of this study confirm that children do not consume enough total fluid according to the recommendations. In addition, children should consume more fluid through beverages than foods, as observed in this study. Although water was the most commonly consumed of all beverages, it is necessary to increase its share in daily beverage consumption, as it currently accounts for only slightly more than one-third of beverage consumption. It has been estimated that food remains the main source of energy and added sugars in children's diets. However, it is important to reduce the consumption of soft drinks, which contribute the most to the intake of added sugars from beverages.
Author Contributions: Concept and design of the study: A.I., M.B., R.B. and I.C.B.; conducting of the study: A.I.; analysis and interpretation of the data: A.I.; drafting of manuscript: A.I., I.R. and M.B. All authors critically analyzed and gave final approval to the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding: This study was funded by the European Commission – Horizon 2020 (Call H2020-SFS-2015-2, Topic: SFS-20-2015, Type of action: RIA, Proposal Number: 678024-2) as part of the project “Strengthening European Food Chain Sustainability by Quality and Procurement Policy” (Strength2Food). The work of doctoral student A.I. was supported by the Croatian Science Foundation through the project “Young researchers' career development project – training of doctoral students” (DOK-01-2018), funded by the European Social Fund.
Acknowledgments: The authors would like to thank the parents, teachers and school staff for their cooperation and support in collecting data for this study. In addition, the authors would like to thank volunteers Lucija Marić, MSc of Nutrition, and Tea Karlović, graduate student in Nutrition at the Faculty of Food Technology and Biotechnology, University of Zagreb, for their assistance in data collection.
Conflicts of Interest: The authors declare no conflict of interest.